Summary of the safety profile: The most frequently reported adverse reaction during treatment is hypoglycaemia. The frequencies of hypoglycaemia vary with patient population, dose regimens and level of glycaemic control, please see Description of selected adverse reactions as follows.
At the beginning of the insulin treatment, refraction anomalies, oedema and injection site reactions (pain, redness, hives, inflammation, bruising, swelling and itching at the injection site) may occur. These reactions are usually of transitory nature. Fast improvement in blood glucose control may be associated with acute painful neuropathy, which is usually reversible. Intensification of insulin therapy with abrupt improvement in glycaemic control may be associated with temporary worsening of diabetic retinopathy, while long-term improved glycaemic control decreases the risk of progression of diabetic retinopathy.
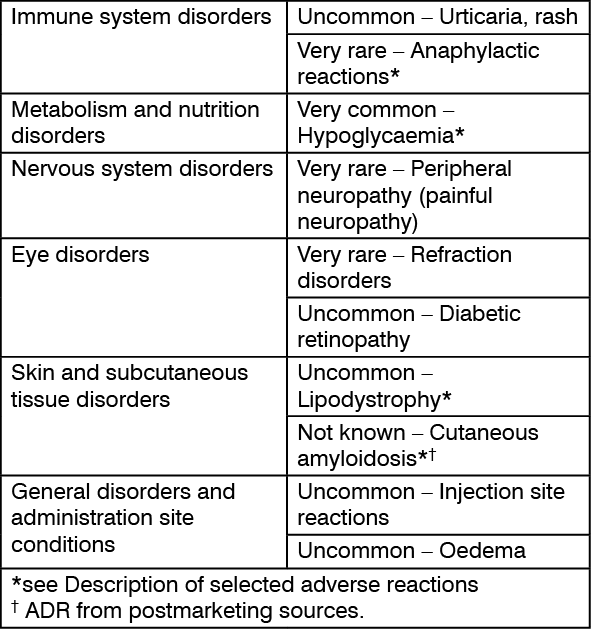
Tabulated list of adverse reactions: The adverse reactions listed as follows are based on clinical trial data and classified according to MedDRA frequency and System Organ Class. Frequency categories are defined according to the following convention: Very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000); not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions: Anaphylactic reactions:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Anaphylactic reactions: The occurrence of generalised hypersensitivity reactions (including generalised skin rash, itching, sweating, gastrointestinal upset, angioneurotic oedema, difficulty in breathing, palpitation and reduction in blood pressure) is very rare but can potentially be life threatening.
Hypoglycaemia: The most frequently reported adverse reaction is hypoglycaemia. It may occur if the insulin dose is too high in relation to the insulin requirement. Severe hypoglycaemia may lead to unconsciousness and/or convulsions and may result in temporary or permanent impairment of brain function or even death. The symptoms of hypoglycaemia usually occur suddenly. They may include cold sweats, cool pale skin, fatigue, nervousness or tremor, anxiousness, unusual tiredness or weakness, confusion, difficulty in concentrating, drowsiness, excessive hunger, vision changes, headache, nausea and palpitation.
In clinical trials, the frequency of hypoglycaemia varied with patient population, dose regimens and level of glycaemic control.
Skin and subcutaneous tissue disorders: Lipodystrophy (including lipohypertrophy, lipoatrophy) and cutaneous amyloidosis may occur at the injection site and delay local insulin absorption. Continuous rotation of the injection site within the given injection area may help to reduce or prevent these reactions (see Precautions).
Paediatric population: Based on post-marketing sources and clinical trials, the frequency, type and severity of adverse reactions observed in the paediatric population do not indicate any differences to the broader experience in the general population.
Other special populations: Based on post-marketing sources and clinical trials, the frequency, type and severity of adverse reactions observed in elderly patients and in patients with renal or hepatic impairment do not indicate any differences to the broader experience in the general population.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out